


A good maxim can go a long way. As part of recent efforts – especially in the United States – to raise the national minimum wage, a particular refrain has found popularity among activists. It goes along the lines of ‘if your corporation cannot afford to pay its employees a living wage, then you do not have a viable corporation’. This adage can be usefully reinterpreted for anyone who cares about scientific skepticism, and untangling misinformation more broadly: if your argument cannot afford to acknowledge better evidence, then you do not have a viable argument.
If your argument can’t survive without shutting its eyes to vast amounts of much stronger, contradicting research – and if your argument can only exist by ignoring vital pieces of information – you don’t have an argument at all. You have a hunch. Wholly unmoored from reality, and dissolving on contact with scrutiny. And, of course, when such ‘arguments’ are accompanied by grand pronouncements of self importance, it should cause our already raised eyebrows to strain ever-higher.
Dr Aseem Malhotra wants you to know that his recent paper is ‘perhaps the most important work of [his] career so far’, that it has ‘survived a rigorous and long peer review process’, and that the paper’s findings have ‘implications for every human being on the planet’. His paper – ‘Curing the pandemic of misinformation on COVID-19 mRNA vaccines through real evidence-based medicine’ – purports to demonstrate (‘reluctantly’ of course) that the mRNA vaccines for COVID-19 carry a knowingly under-reported risk of heart complications with them, and have caused ‘unprecedented harms’. He believes that the Pfizer vaccine contributed to his own elderly father’s death, that vaccine-rollout may be doing ‘more harm than good’, and that it should be suspended immediately ‘pending an inquiry’. His announcement video accompanying the paper surpassed a million views in a matter of days, and vaccine-critical pundits certainly seem excited about it.
Various claims regarding the safety and so called ‘side-effects’ of Covid vaccines, such as ‘vaccine shedding’ and ‘biomagnetism’, have existed as long as the vaccines themselves, despite being entirely unfounded. Scaremongering about ‘gene-altering’ mRNA technology has persisted at every turn, despite relentless debunking. And, of course, baseless vaccine alarmism has a long, loud and inglorious history that predates COVID-19 by several hundred years. And, while the pandemic certainly seems to have sparked something of a renaissance in fear mongering and fringe science, it seems that ideas about ‘microchipping’ and ‘5G’ have been relegated to the dim archives of ridicule, with even hardline covid-’sceptics’ steering clear of, and very occasionally mocking, those particular talking points.
Concerns about heart complications, however, appear to be slightly more salient in the public consciousness, or at least not quite as instantly and recognisably preposterous. Perhaps this is abetted by our memory of the AstraZeneca vaccine being associated with an exceedingly rare risk of blood clotting, resulting in a deliberation between vaccine safety experts and public health officials, and leading eventually to an alternative vaccine being preferentially offered to those in the highest risk age group, even though there is still good reason to believe that blood clots are far more likely to occur from COVID-19 than the vaccine itself. Vaccine-critical pundits have yet to offer a compelling reason as to why ‘Big Pharma’ chose not to cover up this very rare side effect, given that sweeping vaccine injuries under the rug is supposedly their modus operandi.
It is easy to imagine how all of this could contribute to a general, gut-level wariness around vaccination, though. Especially when it comes to cardiovascular issues. Trust in public health has been undermined substantially throughout the pandemic, irrespective of the administration at the helm of the executive branch. Irresponsible government messaging has done considerable damage to the public patience and, unfortunately, feelings of suspicion and unease create an ideal breeding ground for false answers, and those who peddle them.
So the question, then, becomes about how best to respond to these false answers. I firmly believe that, no matter how correct we feel we are, hurling self-satisfied insults at scared, fearful people can only ever be an actively counter-productive affair. The knee-jerk dismissal and puerile ridiculing of all doubts felt by a confused, hurting public will only serve to push them further away and, in many cases, nudge them off the precipice of the rabbit hole they are teetering on.
Whether we like it or not, sizable chunks of the general public are feeling mistrustful. The sheer amount of noise and attention that Dr Aseem Malhotra has managed to galvanise in recent weeks and months bears this out. And the fact that he is ostensibly a ‘highly esteemed, award-winning cardiologist’ who was once a champion of vaccines may well persuade any fence-sitters.
Dr Malhotra’s message is resonating with many. His claims are serious, and his platform is enormous. Which is why it is so important to point out that virtually every single claim that he makes in his paper either misrepresents legitimate sources, accurately represents terrible ones, or demonstrates a foundational misunderstanding of how vaccines actually work. The wider body of high-quality research on this topic is conspicuously absent from his paper, as most of it demonstrates the exact opposite of what Dr Malhotra is trying to argue. His paper is riddled with basic errors, conflicts of interest, unsubstantiated personal anecdotes, telling omissions, outdated anti-vax tropes, logical non-sequiturs, outright mistakes, and dubiously ‘hidden’ extra authors. Absolutely nobody should take this paper as evidence for anything at all. Except, of course, as evidence that Dr Malhotra has a hunch.
The Paper
Dr Malhotra announced his paper to the world by proclaiming that it had ‘survived a rigorous and long peer review process’. Scientists and authors of scientific papers typically do not proudly announce that their work has undergone peer-review, as this is the baseline standard for all real science, and nothing to brag about. Scientists typically let the quality of their work speak for itself. Even the word ‘rigorous’ is bizarrely tautological. All peer-review ought to be rigorous. Proudly declaring that your work has undergone peer-review is like a Broadway dancer gloating about having purchased a pair of shoes. Or an airline pilot insisting to his passengers that he definitely, totally, 100% knows how to fly the plane.
But let’s give Dr Malhotra the benefit of the doubt, and approach this paper with an open mind. If his work has indeed survived peer review, we should expect it to be of the highest quality. Or, at the very least, not to contain any truly glaring errors, which even a non-rigorous peer-review would have spotted.
So, what sorts of things would a peer reviewer be looking for in a paper like this? Well – at the outset, the paper calls itself a ‘narrative review’. NR’s are non-clinical papers, and they tend to be a written summary of all the research that has been previously published on a particular topic. The design of an NR depends on its author, and the objective of the review. Despite having a generally looser protocol structure, they will still usually outline their methods and approaches, while respecting any conventions typically followed in the field they are investigating.
In Dr Malhotra’s review however, there does not seem to be any actual ‘method section’ or given methodology at all. Under ‘methods’, the approach is simply described as a ‘narrative review of the evidence’. It isn’t clear whose narrative is being investigated, nor are any research questions plainly identified. This can be a bit of a red flag, as it suggests that good research discipline is not at the forefront of the author’s attention, and they may be picking and choosing which methodological imperatives to abide by as and when it suits them…
But anyway, all good review articles aim to be an objective and comprehensive analysis of the total current knowledge about a specific area of study, with a view towards establishing a theoretical framework or a contextual focus for that topic. Which means that, in addition to making sure that a paper’s claims are in fact supported by its cited references, peer reviewers of NR’s would need to make sure that the paper does indeed cover all of the key relevant literature on its chosen topic, and that no major studies have been left out simply because they happen to go against the author’s desired narrative. Failing to include inconvenient studies from your analysis, as we all know, is called ‘cherry-picking’.
But perhaps the first thing that a peer reviewer would be on the lookout for is to make sure the paper itself fits the scope and focus of the journal it’s being published in. Different journals may have different remits, and it is often the job of the peer-reviewer to assess how appropriate a paper is for publication. This is where we encounter our first problem. Or, rather, where Dr Malhotra ought to have encountered his.
Dr Malhotra chose to publish his paper on vaccine injuries in… The Journal Of Insulin Resistance. If you’re wondering what on earth vaccine injuries have to do with insulin resistance, the answer is nothing at all. The word ‘insulin’ appears a total of four times in the entire paper (the first of which is crowbarred in at the end of the opening summary). A paper this jarringly out of place would usually lead to a rejection, and the fact that it hasn’t is quite perplexing. The journal itself also seems quite questionable; it does not show up on Pubmed or WebMD, it seems to avoid any quality review, and has published a total of only 30 times since its inception in 2016 (more than half of these are authored by the journal’s own editors, and some are corrections).
On the face of it, it’s difficult to understand why Dr Malhotra would choose such an obscure journal (based in South Africa) to publish ‘the most important work of [his] career so far’. That is, of course, until you take a quick look at the journal’s editorial board, and you see that one of the nine people currently sitting on the board is… Dr Aseem Malhotra.
This is a huge red flag. Being a board member of the very journal that is publishing your work is a dreadfully basic conflict of interest, and one that is never disclosed in Dr Malhotra’s paper. It encourages the unfortunate suspicion that Dr Malhotra’s paper may have not undergone the water-tight peer review process that he claims.
Another unfortunate red flag that occurs at the outset of the paper is the way that Dr Malhotra brings up the tragic death of his elderly father as ‘a case study’. His father:
{who} had taken both doses of the Pfizer mRNA vaccine six months earlier, suffered a cardiac arrest at home after experiencing chest pain… Given that he was an extremely fit and active 73-year-old man… This was a shock to everyone who knew him, but most of all to me… I couldn’t explain his post-mortem findings.
Examining case studies can be both useful and common practice in research. What is less common is for the case study to be an immediate family member of the author, for the issue at hand to be their tragic death, and then for the conflict of interest statement to claim that the author has ‘no personal relationships that may have inappropriately influenced them in writing this article’. Including a personal anecdote in a narrative review becomes questionable when we know, due to the PR around the paper’s release, that Dr Malhotra explicitly attributes his father’s death to the vaccine. But this, of course, is an empirical claim, requiring proof like any other. We shall see if Dr Malhotra provides it over the course of his paper.
Even more unpromising is the fact that Dr Malhotra begins his paper by reminding us all of a previous occasion in which he cherry-picked studies for a piece he authored in the British Journal of Sports Medicine. He claims that his previous ‘high impact, peer reviewed paper’ (though it is actually an opinion editorial) represented ‘the best available evidence’ on how to ‘delay the progression of heart disease’ via ‘lifestyle changes’, while neglecting to mention that it was roundly criticised for misrepresenting data, and failing to include ‘the totality of the evidence base’ by leaving out ‘well acknowledged, higher quality’ literature from his analysis, in favour of ‘methodologically weak, low quality research’. In other words, Dr Malhotra ignored better evidence, because that better evidence did not fit his desired narrative.
Unfortunately, it looks like this incident was not a one-off. Dr Malhotra’s abrupt change of heart on vaccines may seem a little out of the blue to those unfamiliar with his background, which happens to be one of controversial diet advice. His book ‘The Pioppi Diet’ was called one of ‘the top five worst celeb diets to avoid in 2018’ by the British Dietetic Association, and his views on saturated fats have been widely criticised as oversimplified, unfounded and based on cherry picked research. He has attempted to dispute the efficacy of statins, and the influence of cholesterol, on heart disease – both of which are at odds with the broader medical consensus, and have been described as misleading and dangerous to public health. Oxford medical professor Rory Collins warned that such baseless scaremongering around statins had the potential to cause even more harm than Andrew Wakefield’s MMR vaccine paper.
When viewed like this, the metamorphosis from diet guru to vaccine-critic might seem less like ‘a fall from grace’ and more like a rather unsurprising sideways career move. But notably, Dr Malhotra responded to these substantive criticisms of his work from the medical community by lashing out at the BDA and the BHF, and denouncing them as ‘hired hands’ that curry favour for the food industry. He has called Public Health England ‘a front group for the processed food industry’ after they dared to criticise his book. Responding to critics by lambasting them as corporate puppets, it seems, is a tactic Dr Malhotra resorts to over and over and over again.
Now, a cynic might point out that the veritable ocean of red flags here doesn’t instil the greatest confidence in Dr Malhotra’s academic bona fides. And while I think it is fair to say that recounting the time a bunch of scientists condemned your work as being cherry-picked isn’t the best way to kick off a narrative review, let’s give Dr Malhotra the benefit of the doubt (again) and approach his new paper with an open mind (again). Giving opposing views an honest hearing is a charge we take on proudly at The Skeptic. Let us allow Dr Malhotra the chance to present his case. Surely, no principled scientist would make sweeping claims with enormous confidence unless they had robust research to back it up.
Stunningly though, within the first few paragraphs of the paper, Dr Malhotra goes on to mistakenly reference the wrong study he is quoting from. Under the heading ‘Questioning the data’, he incorrectly cites this paper as containing data in the supplementary appendix showing that there were ‘four cardiac arrests in those who took the vaccine versus only one in the placebo group’. The cited paper shows no such thing, and peer-review did not catch the blunder. The cited paper actually shows four deaths in the placebo group, and two in the vaccine group.
The paper Dr Malhotra likely meant was this one, which is a follow up of the original trial – in the same journal – containing the data for six months, and it does contain the figures he mentions in the supplementary appendix. There were indeed four cardiac arrests in the vaccine group versus one in the placebo group. However, there were also two deaths from myocardial infarction in the placebo group, and none in the vaccine group. The same numbers can be seen for pneumonia, and multiple organ dysfunction syndrome. It’s difficult to infer much at all from numbers this marginal. Dr Malhotra’s penchant for oversimplification might be clouding the fact that ‘cardiac arrest’ is actually only one of twenty-six causes of death the data accounts for. And given that he explicitly mentioned myocardial infarction (heart attack) in his list of injuries supposedly caused by the vaccine, it is puzzling that the very source he is quoting from appears to completely contradict this assertion.
Dr Malhotra also initially references the infamous Abstract 10712 paper as the article which piqued his initial interest in this topic. The abstract was published in Circulation, and has a giant expression of concern placed on it due to ‘several typographical errors’ and the fact that ‘no statistical analyses for significance was provided, and the author is not clear that only anecdotal data was used’, which could mean that the study ‘was not reliable’. The paper itself even states that the ‘data has not been validated’ and ‘no statistical comparison was done in this observational study’. And while Dr Malhotra does admit that there were ‘early and relevant criticisms’ of the paper, he does not outline any of the above faults specifically – rather, he goes on to say:
… but nevertheless, even if [the findings were] partially correct, that would mean that there would be a large acceleration in progression of coronary artery disease, and more importantly heart attack risk.
Speculating about what a fatally flawed study would mean were it not fatally flawed is a highly unusual way of opening a narrative review. Holding up a piece of definitively terrible research (by its own admission) and saying ‘ah, but even if it were partially correct…’ is a baffling approach for any scientific venture.
It is difficult, of course, to infer much at all from studies as defective as the Circulation Abstract, or from numbers as small as those in the NEJM supplementary appendix. It’s hard to see why Dr Malhotra included them in the first place, or what this could possibly achieve. Apart from seeding the idea in reader’s minds that something feels a little fishy here… Again, attempting to implant the ominous beginnings of a hunch in your readers is a highly unorthodox approach for a review article.
A much better way of finding out whether or not the vaccine is causing an increase in heart attacks would be to simply take a look at any of the numerous, large scale, reputable studies that have been carried out examining this very question. Come to think of it, doing so would be entirely appropriate for what is supposed to be a narrative review paper. The bare minimum, some might say.
So… Let’s do that, shall we?
A study published in the New England Journal of Medicine, used data from the largest health care organisation in Israel, and it compared the rate of adverse events following vaccination or infection with Covid with the rate in unvaccinated/uninfected controls. It found that there was no increase in myocardial infarction, pulmonary embolism, deep-vein thrombosis, pericarditis, arrhythmia or intercranial haemorrhage in vaccinated groups, but some increase in myocarditis, lymphadenopathy (swollen lymph glands), appendicitis, and herpes zoster infection (shingles). In contrast, SARS-CoV-2 infection was associated with an increase in every single one of the aforementioned adverse events, plus a greater increase in myocarditis.
A study published in JAMA, used the French National Health Data System to look at the incidence of myocardial infarction, stroke and pulmonary embolism in 3.9 million vaccinated people aged 75 or over. They found there was no increase. Another study published again in JAMA, used the Korean nationwide COVID-19 registry and the Korean National Health Insurance Service database to compare the incidence of acute myocardial infarction and ischemic stroke after covid infection in vaccinated and unvaccinated groups, with a cohort of just under a quarter of a million people. They found that the incidence of both was higher in those that were unvaccinated. A study published in Cardiovascular Research, examined the association between vaccination and major adverse cardiovascular events (MACE) in 229,235 individuals with cardiovascular disease. They found no evidence of increased risk of MACE after vaccination.
Each of these large-scale studies were published in reputable, well acknowledged journals, freely available to both Dr Malhotra and his peer reviewers, and they examined precisely the questions Dr Malhotra is asking. But instead of including these (or dozens of other studies like them) Dr Malhotra chose to begin his review paper with a personal anecdote, a previous article of his that suffered from cherry picking, and an infamously flawed abstract that tells us nothing at all. Why did peer review think this was appropriate?
Dr Malhotra’s fondness for peculiar sources doesn’t stop there. One of the very first tables of data to appear in his paper is sourced from an online blog. Another table appears alongside it, which comes from John Ioannidis, who has spent much of the pandemic making unsubstantiated claims over and over and over again. Citing him uncritically is a red flag.
Blog posts are not reputable sources, and do not belong in a scientific paper. Let alone a blog post from the website for Health Advisory & Recovery Team (HART), whose co-founder believes in treating autism with homeopathy, and whose board members have an atrocious record of promoting wild conspiracy theories (including baseless claims of vaccine-induced magnetism, vaccine-induced autism, vaccine-induced fertility damage, 5G/nanotech, mass gene-therapy, earth depopulation, referring to vaccines as ‘bioweapons’, talk of ‘Nuremberg’-related consequences for nurses caught administering the vaccine…) according to leaked chat logs from within the group itself.
The fact that Dr Malhotra chooses to pull figures from a dubious online blog instead of any national health database seems inexplicable, until we glance at the acknowledgements section at the end of his paper, which thanks an uncredited, extra author for behind-the-scenes ‘edits and analysis’. In this case, that author is Dr Clare Craig, a member of HART (who herself often misrepresents data, and once encouraged other HART members to ‘seed the thought that vaccines cause covid before asking the second question of whether that means there is an overall benefit or not…’). Collaborating with an uncredited co-author is itself unusual, let alone one with such close ties to anti-vax disinformation groups.
Malhotra then makes a familiar old argument about how the ‘Absolute Risk Reduction’ in the Pfizer trials was actually alarmingly small compared to the ‘Relative Risk Reduction’, and that this scandalous fact should’ve been made clear to the public in the name of ‘transparency’ and ‘informed consent’.
This has been a common talking point in anti-vax circles for a very long time, and has been repudiated thoroughly over and over again. Dr Malhotra’s peer reviewers clearly did not feel the need to point any of this out.
Dr Malhotra goes on to make further claims that are, in fact, directly contradicted by the very references he uses to support them. He writes that:
Contrary to popular belief, what the trial did not show was any statistically significant reduction in serious illness or COVID-19 mortality from the vaccine over the 6-month period of the trial, but the actual numbers of deaths (attributed to COVID-19) are still important to note. There were only two deaths from COVID-19 in the placebo group and one death from COVID-19 in the vaccine group.
The source he cites here, again, shows no such thing. Instead, the document – an FDA clinical review – shows a 96.7% reduction in severe cases of infection (which is absolutely statistically significant), and it showed six deaths from COVID-19 in the placebo group, and only one in the vaccine group. A far cry from the numbers quoted by Dr Malhotra. Is he misrepresenting the figures on purpose? Or did he simply not read the document he is quoting from? Moreover, if Dr Malhotra is interested in the vaccine’s effect on COVID-19 mortality, it is quite mystifying why he didn’t simply take a look at the shelves of data now available on this very subject.
He then incorrectly claims that a paper in Nature revealed that there was:
…a 25% increase in both acute coronary syndrome and cardiac arrest calls in the 16- to 39-year-old age groups significantly associated with administration with the first and second doses of the mRNA vaccines but no association with COVID-19 infection.
The paper in question (which is actually in Scientific Reports not Nature) comes with a large expression of concern at the top, due to ‘criticisms that are being considered by the Editors’. These criticisms concern clinically irrelevant correlations, basic statistical errors, and flawed methodological approaches. A paper like this cannot tell us very much, and is quite inappropriate for a narrative review.
Baffling logical errors pervade Dr Malhotra’s paper too. He uses work by Fenton et al. to offer a possible explanation for the increase in mortality being seen in unvaccinated people. He writes:
A rise in mortality after vaccination [could have been] misattributed to the unvaccinated population: in other words, those counted as ‘unvaccinated deaths’ would in fact be those who had died within 14 days of being vaccinated.
As evidence for this claim, he writes that:
… a freedom of information [FOI] request has now confirmed that authorities in Sweden were indeed categorising deaths within 14 days of dosing as unvaccinated, creating a misleading picture of efficacy vs death
I probably don’t need to spell this out, but… in order to prove that something is happening in England, you need to prove that it is happening in England. Not that it is happening in Sweden. This is a complete non-sequitur, and doesn’t prove what Dr Malhotra is arguing in the slightest. Furthermore, the ONS in the UK makes it clear that:
An unvaccinated individual is someone who has received no vaccinations.
For the purposes of their statistics, once you have been vaccinated, you are considered ‘vaccinated’. And if we are talking about Sweden, it is worth mentioning that despite having a higher vaccine uptake than the US and a higher booster uptake than the UK – with half of all 12-17 year-olds vaccinated – they are seeing no significant rise in excess deaths:
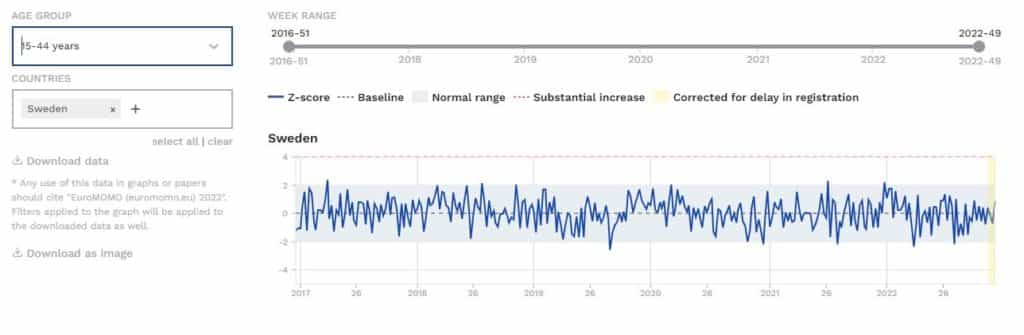
Sweden is even seeing negative excess deaths among the young, despite very high vaccine uptake. If Dr Malhotra has any theories as to why these supposedly ‘unprecedentedly’ harmful vaccines are choosing to spare Sweden, I’d love to hear them. Perhaps the spike protein’s pathological influence wanes substantially upon exposure to ABBA. A dubious theory, perhaps, but nevertheless – even if partially correct…
Speaking of which, Dr Malhotra also seems to demonstrate a basic misunderstanding of how vaccines work at all. In speculating about what the ‘mechanism of harm’ could be, he writes that:
For ‘conventional vaccines’, an inert part of the bacteria or virus is used to ‘educate’ the immune system. The immune stimulus is limited, localised and short-lived. For the COVID-19 vaccines, spike protein has been shown to be produced continuously (and in unpredictable amounts) for at least four months after vaccination.
Dr Malhotra appears to have never heard of ‘live attenuated vaccines’, which have been around for hundreds of years and use versions of ‘living’ viruses, rather than inert parts of the virus. And, of course, the reference that Dr Malhotra provides in support of the ‘unpredictable’ spike protein claim shows nothing of the sort.
When discussing the incidence of vaccine-induced myocarditis in young adults, under the subtitle ‘What are the harms?’, he writes that:
Although vaccine-induced myocarditis is not often fatal in young adults, MRI scans reveal that, of the ones admitted to hospital, approximately 80 % have some degree of myocardial damage. It is like suffering a small heart attack and sustaining some – likely permanent – heart muscle injury. It is uncertain how this will play out in the longer-term…
As ever, the grave undertones of Dr Malhotra’s statements are somewhat undercut by the very literature he uses to support them, which reads:
Patients with vaccine-associated myocarditis… demonstrated rapid clinical improvement with no adverse events over short-term follow-up.
That’s certainly a far cry from ‘it’s like a small heart attack’ and ‘likely permanent muscle damage’. Of course, exaggerating the so-called ‘harms’ of the vaccine, while minimising the harms of COVID-19 itself, is a long-standing manoeuvre in covid casuistry, and it’s certainly a recurring theme in Dr Malhotra’s paper. But again, it’s simply not borne out by the vast amounts of better evidence. If he had simply glanced at some of the large-scale, high quality research pertaining to vaccine-induced myocarditis – such as this NEJM study, which found that it was ‘rare, mild… and benign over a follow-up period of six months’ (even in the highest risk age group) – his alarm might’ve been assuaged.
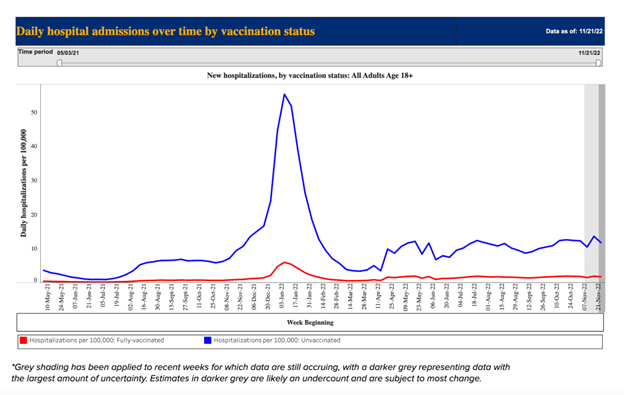
Dipping into the wider body of evidence on virtually all of Dr Malhotra’s claims may well have given him some much needed solace. ONS data shows that ‘sudden cardiac deaths’ were down in 2021 compared to the previous five years, and that mortality is, unfortunately, higher in the unvaccinated. Research published by JAMA shows that The US States with the highest vaccination rate have the lowest mortality rate, and vice versa. Further research shows that even non-Covid mortality is lower following vaccination across all age groups (and across race and sex). Myocarditis is far more likely to occur after COVID-19 infection than vaccination, and the latter is often mild (as Dr Malhotra himself once argued…)
Any excess mortality that is occurring is extremely unlikely to be traceable to the vaccine. As a matter of fact, a rise in all-cause excess mortality has been observed in the aftermath of many pandemics and epidemics throughout history. The 1918 influenza pandemic (for which there was no vaccine) saw an increase, which did not return to baseline until several decades later. In terms of cardiac deaths, they were already on the rise during year one of the Sars-CoV-2 pandemic (before the vaccine was around), which were attributable directly to COVID-19 infection. Those infected had higher rates of cardiac problems within the following year, including blood clots. All of which, it should be said, the vaccine is protecting against phenomenally well:
For someone so interested in vaccine injuries, Dr Malhotra demonstrates a lack of curiosity about what the actual research says on the matter. It’s not as if these studies are difficult to find. They are, almost all of them, published by internationally acknowledged journals, whose names are readily familiar to any scientist (unlike The Journal of Insulin Resistance), and they are all directly germane to his field of interest.
Dr Malhotra chooses instead to use ominous anecdotes and emotionally loaded language to foster a sinister inkling in his readers, making them more likely to overlook the little inaccuracies in his analysis, and less likely to check his sources. Conspiratorial suspicions often encourage a particularly relentless kind of confirmation bias, where data inconsistencies don’t matter and eerie coincidences do. A hunch can be a powerful thing.
But narrative reviews aren’t supposed to feel like a whodunnit. They are supposed to be an objective analysis of all the key, relevant research around a topic, irrespective of whether or not they fit your hunch. If you are unwilling or incapable of looking at a wider portfolio of evidence, you may not be ideally suited to authoring a narrative review.
One thing should be very clear by now. If there exists any compelling evidence that vaccines are causing ‘unprecedented harm’, it is not present in this paper. Almost no good quality evidence is. If this paper represents the best that the vaccine-critical movement has to offer, they do not have a leg to stand on. Dr Malhotra consistently distorts the findings of reputable studies, overstates the findings of dreadful ones, and omits everything else. This is not standard, scholarly practice. By extension, every single reporter and journalist that amplified this paper in order to foment vaccine-hesitancy is, in effect, publicly declaring that they do not care about good evidence. I suppose, in this way, we should all be indebted to Dr Malhotra for providing us with this rather handy litmus test for the integrity of pandemic pundits.
Needless to say, at no point in the rest of his paper does Dr Malhotra ever offer any further evidence that the vaccine contributed to his father’s death. We are simply enjoined to take his word for it, and inflame our own hunches. Although, amazingly, he does dedicate a later section to railing against ‘biassed reporting in medical journals’. Irony, it seems, did survive the peer review process.
The interviews and appearances Dr Malhotra has given in the aftermath of his paper’s publication leave no doubt about his new career path, and his newfound ideological bedfellows. The infamous Steve Kirsch hosted Dr Malhotra at a VIP dinner event in Texas, alongside Peter McCullough. Tickets began at $150, and went up to $500 for a ‘private meet-and-greet cocktail reception’. In addition to appearing on GB News and Tucker Carlson Today, Dr Malhotra has also given interviews to Del Bigtree and Children’s Health Defence, both of whom have spent years promoting Andrew Wakefield’s spurious claims about the MMR vaccine and autism. (Dr Malhotra himself lamented the “very worrying” reduced uptake of the MMR vaccine in recent years, despite simultaneously working with the very groups that campaign most ferociously for this exact goal).
Most appallingly of all, Dr Malhotra promoted a video that attributed the death of a 15-year-old child to the vaccine, when the child in question was not even vaccinated. She died of a complication associated with COVID-19 infection on the day she was due to get her first dose of the vaccine, having tested positive four days previously. Misrepresenting the death of a child is, even by anti-vax standards, breath-taking.
But perhaps the most telling moment came from a panel appearance at an event hosted by the World Council for Health (itself a hotbed of 5G conspiracy theory and anti-vax sentiment). In the Q&A section near the end of the event, at around the 2:27:57 mark, an audience member asks Dr Malhotra if he ‘still believes in airborne viruses’ at all. After a brief, awkward pause he laughs – nervously – and then passes the microphone to another panellist. Watching him sit there, shifting uncomfortably in his seat as the moderator attempted some kind of answer, I couldn’t help but feel that perhaps Dr Malhotra is just a little bit unsettled by his new fanbase.
Perhaps even the ‘highly esteemed, award-winning* cardiologist’ Aseem Malhotra feels a little out of his depth in the wild new world he has entered. Perhaps, on some level, he didn’t fully know what he was getting himself into. Maybe someday, years down the line, this very moment will constitute the basis of another change of heart. Perhaps Dr Malhotra will eventually see the error of his ways, recognise the seismic flaws in his analysis, and commit himself to a higher standard of scholarly practice. The world of woo is full of defectors, after all. Who knows? There may yet come a day when Dr Malhotra joins the ranks of those who regret having turned a blind eye to better evidence, and admit when they were wrong.
… But I have a hunch he won’t.
*In a now deleted tweet, Dr Malhotra claimed he was ‘truly honoured to receive the Champion of Preventative Medicine award from the Chair of the BMA, Chaand Nagpaul’. Both the BMA and Chaand Nagpaul deny having given him an award.