


Chronic disease is having a moment in the political spotlight. This is especially true in the United States where it has become a favorite talking point of Secretary of Health and Human Services, Robert F. Kennedy Jr. Statements like his seemingly baseless claim that only 3% of the US population had a chronic disease during his uncle’s presidency may be easy to dismiss. More problematically, his assertion that prevalence of chronic disease is on the rise, and the CDC’s figure that 90% of US health expenditures are for people with chronic and mental health conditions, are broadly true.
What qualifies as a chronic disease – sometimes used interchangeably with ‘non-communicable disease’ – varies, but it is generally any long-lasting illness that requires continuing care, with some definitions specifically excluding infectious diseases. In the US, 8 of the 10 leading causes of death in 2023 were related to chronic disease, including heart disease, cancer, and stroke. That chronic disease accounts for so many deaths in the US may seem to paint a dismal picture for population health, however this fact must be viewed in the proper context, to fully understand the landscape of health in a developed nation.
The Epidemiological Transition
The Epidemiological Transition is a theory that was first proposed in 1971 by Abdel Omran. It describes how, as a country develops, advancements in healthcare and public health allow it to better treat and prevent infectious disease, significantly lowering their mortality. This drives increases in lifespan, which allows more time for people to develop chronic diseases whose mortality occurs on a longer timescale.
At the time of writing, we have not yet discovered the secret to immortality. Everyone will die from something. The longer somebody lives and the better we are at managing infectious disease, the more likely it is that they will die, at least in part, from a chronic disease. It is therefore not inherently a bad thing that so many of the leading causes of mortality are chronic diseases; it can be seen as a sign of how adept our public health and healthcare infrastructures have become in controlling some of the greatest historical threats to human life.
With that in mind, let’s look at the claim that 90% of US health expenditures are for people with chronic and mental health conditions. This figure comes from a 2017 chartbook from the Rand Corporation titled ‘Multiple Chronic Conditions in the United States’. The first issue is that the 90% figure refers to care for people who have chronic and mental health conditions, not necessarily care for those conditions. While it also establishes that people with these conditions do use health services more, the 90% figure does not tease out the expected baseline cost of care.
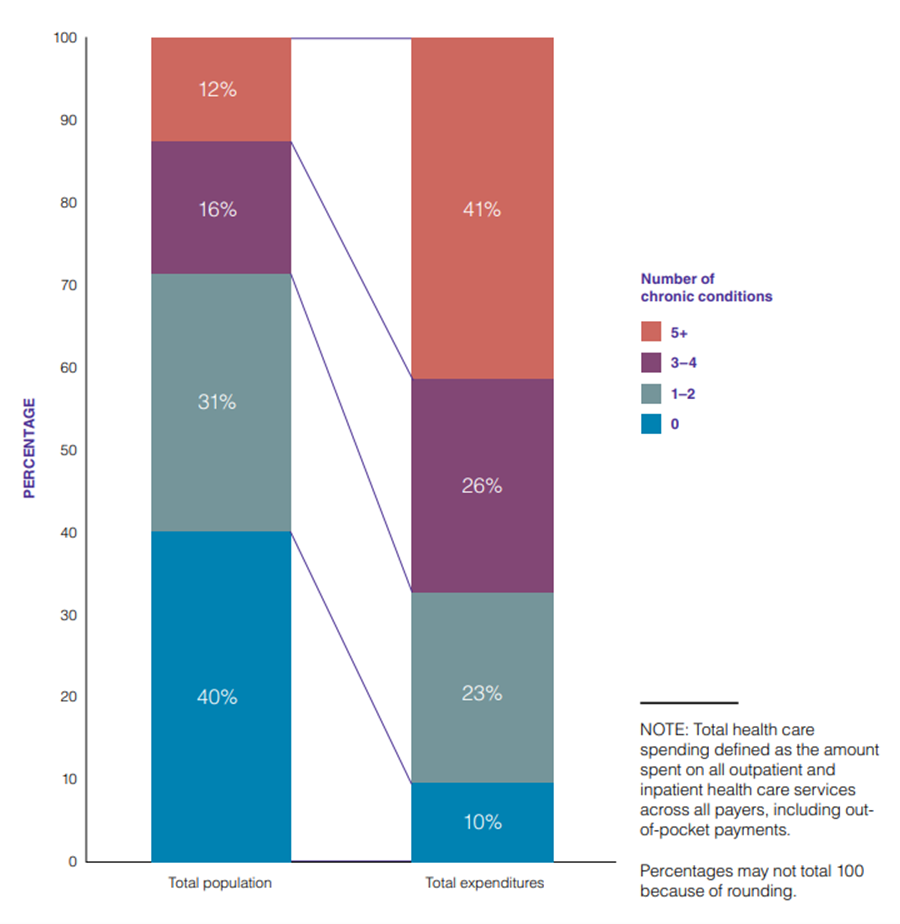
This figure also requires the context of what percentage of people have chronic or mental health conditions. The same chartbook reports that in 2014, 60% of adults in the US had at least one chronic condition, which means 90% of healthcare spending went to care for 60% of adults. They also report that the share of that spending increased based on the number of concurrent chronic conditions, and that having multiple chronic conditions is heavily associated with age. 81% of adults 65 and older had multiple chronic conditions, compared to 42% of adults overall. People with one or two chronic conditions represented 31% of the population, but only accounted for 23% of spending, while people with five or more chronic conditions represented only 12% of the population and whose medical care accounted for 41% of healthcare spending.
Therefore, when we look at that 90% figure in context, we can see how significant an impact age has on healthcare expenditures. This lines up with what we would expect from Omran’s theory of the Epidemiological Transition, and may change how we look at policy and public health efforts to address the underlying challenges.
Prevalence
Prevalence is a measure of disease frequency commonly used when discussing chronic disease. It refers to the total amount of a given disease within a population at a moment in time, like the number of people in the UK who are currently living with type 2 diabetes. While it is an important figure for illustrating the impact of a disease on the population and healthcare infrastructure, it can be counterintuitive.
Kennedy does not provide any evidence for his claim that prevalence of chronic disease was as low as 3% during the John F. Kennedy administration, but it is correct to say that the reported prevalence of chronic disease in the US has risen since the 1960s. While this could be a result of more people developing chronic disease, there are several positive reasons that also contribute to increases in prevalence.
The longer somebody with a chronic disease lives, the longer they are counted in prevalence numbers for that disease. As a result, increases in treatment effectiveness and accessibility can lead to larger prevalence numbers. For example, the yearly number of new HIV infections in the US fell by 73% between 1985 and 2019, but prevalence remains high, with roughly 1.2 million people living with HIV, due to highly effective treatments that significantly extend life expectancy.
Another positive contributor to increasing prevalence is improvements in screening. In 2016, the US Preventative Services Task Force recommended physicians screen adults for depression. After implementing that screening, a large healthcare system in Northeastern Ohio saw depression diagnoses rise from 1.7% of monthly patients to 2.9% of monthly patients. The number of people living with depression did not change, but more of them were being counted and more of them could seek care for the condition.
A similar effect is seen when there are changes in diagnostic criteria. For example, The World Health Organization puts out a set of guidelines called the International Classification of Diseases and Related Health Problems (ICD). A study of 85-year-olds in Gothenburg, Sweden compared how different sets of criteria for classification affected the recognized prevalence of dementia, including using two versions of the ICD. Classifying cases according to the older ICD-10 placed the prevalence at 20.5%, while classifying the same cases using the newer ICD-11 placed the prevalence at 36.4%. As our understanding of disease changes, we may recognise new or early symptoms that widen the scope of diagnosis. Just like with improved screening processes, the real number of people with dementia did not increase, we just got better at recognising the disease.
The reality
Is the prevalence of chronic disease in the US going up entirely because of these positive health advancements and the increasing age of the population? Is all this worrying over chronic disease for nothing? Probably not. The reality is that there have been major improvements in some areas, while others have struggled. While heart disease is the number one cause of death in the US, its mortality fell 66% between 1970 and 2022. However, these advancements in health are not always equitably distributed across the population, and we cannot ignore the mounting economic costs of treatment for chronic diseases where increased prevention efforts could be more effective.
While Kennedy’s stated ethos of strengthening our approaches to prevention is welcome, his actions tell a different story. From halting meetings of the US Preventative Services Task Force, to cutting funding for mRNA vaccine development, it is difficult to see how his policies could ‘make America healthy again’.
Public health has been swimming against a tide of misinformation in the wake of the Covid-19 pandemic, and Kennedy has been a valuable ally for the wrong side of that equation. At the same time, much of the messaging around chronic disease predates his time with Health and Human Services, including the major claims examined in this article. If the field of public health is to preserve credibility in the face of heightened scrutiny and mistrust, it is vital that we put our messaging in the proper context. Our communications must do a better job of walking the line between urgency and fearmongering.