


Paloma Shemirani’s story should deeply disturb us. At 23, she was diagnosed with non-Hodgkin lymphoma, with an approximately 80% chance of cure through chemotherapy. She died seven months later, after refusing conventional treatment and opting for alternatives such as “Gerson therapy” (a combination of restrictive diets, juices, and coffee enemas). Her brothers, Gabriel and Sebastian, believe Paloma died because of the conspiracy theories of their mother, Kate Shemirani, a former nurse turned anti-vaccine influencer and promoter of ‘alternative medicine’.
The BBC’s account of the case is devastating. Kate Shemirani even sent messages in all caps to Paloma’s boyfriend: “TELL PALOMA NOT TO SIGN OR VERBALLY CONSENT TO CHEMO OR ANY TREATMENT.” Hospital staff wrote down their “concern about maternal influence” on the patient, but acknowledged that Paloma had the legal capacity to make her own decisions. A young woman who was gradually convinced that the medicine that could save her was, in fact, her enemy.
This case tragically illustrates a phenomenon I observe frequently. With almost weekly regularity, I encounter comments like “the pharmaceutical industry doesn’t want a cure for cancer to be found” or, even more dramatically, “they even kill those who find the cure”.
These statements are, to some extent, understandable because they stem from a collective distrust of large corporations. The problem is that this almost-skeptical stance ends up being manipulated and directed to fuel misinformation about how medical science works.
What the data shows
To understand the true scale of the problem, we can examine a study published in the journal JAMA Oncology in 2018. Researchers analysed data from nearly 2 million patients diagnosed with curable cancers (breast, prostate, lung, and colon) in the United States between 2004 and 2013, from more than 1,500 accredited cancer treatment centers. They used a methodology that adjusted for variables such as age, clinical stage, comorbidities, insurance type, ethnicity, and cancer type.
In the sample studied, they identified 258 patients who used complementary medicine, specifically defined as “unproven treatments administered by non-medical personnel”, in addition to conventional treatment. This seemingly small number actually reflects the difficulty of documenting the use of these practices, as many patients do not disclose to their physicians that they are using alternative therapies and, when they do, it is not always documented in their medical records.
The results are worrying. Patients who opted for complementary medicine had higher rates of refusal of conventional treatments: 7% refused surgery (compared to only 0.1% of the control group), 34.1% refused chemotherapy (compared to 3.2%), 53% refused radiotherapy (compared to 2.3%), and 33.7% refused hormone therapy (compared to 2.8%).
Most importantly, 5-year survival was 82.2% in the group using complementary medicine, compared to 86.6% in the control group, an absolute difference of 4.4% that, although it may seem modest, represents thousands of preventable deaths when extrapolated to the general population, considering the approximately 700,000 new cases of cancer diagnosed annually in Brazil.
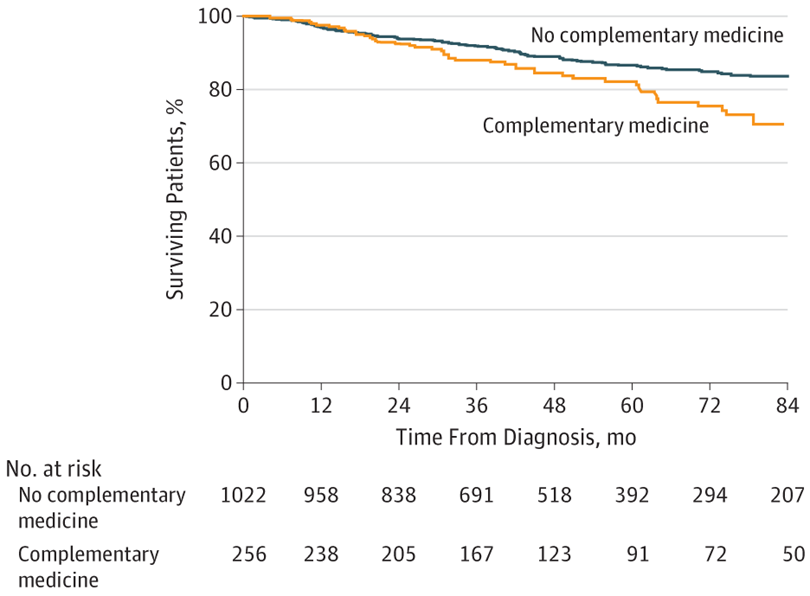
The difference in mortality disappeared when researchers adjusted the data to account for refusal of conventional treatments. In other words, it is not the complementary intervention itself that appears to increase mortality, but rather the systematic tendency of users to refuse treatments with scientifically proven efficacy.
Another interesting aspect of the study was the demographic profile of “complementary medicine” users. Patients who opted for these therapies were, on average, younger, more educated, had better access to private health insurance, and had a higher median family income. A profile similar to that of Paloma Shemirani.
Conspiracy ideas
Let’s return to the phrase I hear almost weekly: “The pharmaceutical industry doesn’t want a cure for cancer to be found”. While it sounds shocking, it ignores the fact that:
1. Many cancers are already cured
Several types of cancer currently have high cure rates. Breast cancer, detected early, has a survival rate of over 90%. Childhood leukemia, which was practically a death sentence just a few decades ago, now has cure rates above 80%. Thyroid cancer has a 5-year survival rate of over 98%. Testicular tumors, even when metastatic (having spread from the original site), have a remission rate of over 90% in cases with a good prognosis. Melanomas detected early have a 99% survival rate.
If there really were a corporate conspiracy to hide cures and keep patients sick indefinitely, how would we explain these widely documented, celebrated, and publicised advances? Is it a curiously incompetent conspiracy, systematically “forgetting” to suppress successes in certain areas while obsessively focusing on others?
Or perhaps it’s simply the naturally uneven and progressive scientific development that characterises all medical research. Some problems are easier to solve than others, some organs are more surgically accessible, some tumors respond better to chemotherapy. It’s biological reality being confused with conspiracy.
2. “Cancer” is not just one disease
Herein lies perhaps the greatest conceptual error fuelling conspiracy theories: the idea that ‘cancer’ exists as a single entity. In reality, the term encompasses more than 200 molecularly distinct diseases, each with its own genetic, behavioural, and therapeutic characteristics, differences amplified by the particularities of each individual’s immune system.
Lung adenocarcinoma is as different from acute lymphoblastic leukemia as the flu is from malaria. Both are ‘diseases’, but their mechanisms, treatments, and prognoses have almost nothing in common. Searching for a “universal cure” for cancer is like searching for a single medicine that simultaneously cures the flu, tuberculosis, malaria, meningitis, AIDS, and syphilis.
3. The economic paradox
Here we encounter a fundamental economic paradox. A company that developed a ‘guaranteed and effective’ cure for just one of the most common cancers would automatically become one of the most valuable corporations in history. The global oncology market is indeed worth billions of dollars annually. A company holding the patent for a revolutionary cure for, say, lung cancer, could charge virtually any price and still have guaranteed global demand.
Why would a corporation voluntarily give up the largest profit in the history of medicine? Conspiracy logic would require all the world’s major pharmaceutical companies –companies that compete fiercely for market share, sue each other for patent infringement, and engage in industrial espionage – to maintain an unbreakable secret pact to forgo trillions of dollars in profits.
4. Who profits from the conspiracy?
Those who profit most from the systematic distrust of conventional medicine are the sellers of “alternative cures.” Kate Shemirani’s case is a perfect case study of what I previously called the Chameleon Lobby: the strategy of using criticism of corporations to shield one’s own questionable business practices.
Kate charges £70 for annual memberships on her website and £195 for individual consultations, selling everything from apricot seeds with “potential health benefits” to personalised 12-week programmes for cancer patients.
The global alternative medicine market also generates billions of dollars annually, growing at rates exceeding 20%. Unproven treatments, “miracle” supplements, pseudoscientific therapies, and “superfoods” thrive because they don’t need to demonstrate efficacy or safety through rigorous studies. It’s a market that operates with stratospheric profit margins (after all, how much does it cost to produce a bottle of “energised water” or a juice-based “detox” program)?

5. Persistence of aggressive treatments
But why, then, do doctors sometimes insist on chemotherapy, even in very advanced cases with bleak prognoses? Why do they continue to offer “another line of treatment” when the chances of benefit are statistically minimal? Is it because they’re serving the industry?
The answer lies in the complex intersection between our collective cultural difficulty in accepting the finitude of life, the still incipient evolution of palliative care in Brazil, and the psychological pressures inherent in medical practice. It is, in fact, a human limitation that reflects the cultural relationship with death. Health professionals are trained to heal, to intervene, to ‘do something‘. The idea that sometimes the best medicine is to not medicate goes against decades of conditioning.
Patients and families, in turn, tend to interpret the lack of active treatment as ‘giving up’ or ‘abandonment’. There is enormous social and emotional pressure to ‘fight to the end’, even when that fight becomes a prolongation of death, not life. This reflects what we’ve already discussed about heroic medicine: the psychological pressure to act, even when the best course of action would be to accept that we’ve reached the limits of what medicine can offer.
6. A real question
There’s a documented and growing problem in modern oncology that deserves serious discussion: overdiagnosis. Increasingly sensitive tests detect cellular changes that technically fall under the definition of ‘cancer’, but would never cause significant clinical problems if left untreated.
These indolent lesions end up being treated as ‘real’ cancer, subjecting patients to invasive procedures, anxiety, costs, and side effects to treat irrelevant diseases.
This is especially true of poorly designed screening programs and the growing epidemic of unnecessary checkups (a phenomenon we already addressed when discussing quaternary prevention). Paradoxically, some of today’s oncology ‘successes’ may reflect this ability to detect and treat cancers that never needed treatment, rather than actual advances in curing clinically significant cancers.
But it’s important to note: this is a real problem that the medical community recognises and is working to correct. And how? Not through conspiracy, suppression of information, or denial, but through open scientific research, transparent discussion of the medical literature, guideline revisions, and continuing professional education.
Final considerations
Cancer conspiracy theories often urge the public to ‘research for themselves’ and ‘question everything’, but they rarely present evidence that stands up to rigorous scientific scrutiny. When specifically questioned about biological mechanisms, statistical methodologies, peer review, or replicability of results, the claims invariably turn out to be based on biased testimony, conceptual misunderstandings, or deliberately fabricated misinformation.
It is a form of performative skepticism: it uses the language and values of legitimate scientific inquiry but selectively, applying asymmetric standards of evidence that require extraordinary evidence for conventional claims and accept minimal evidence for extraordinary claims.
Oncology medicine faces real limitations that deserve honest discussion and constructive criticism: costs that make treatments inaccessible to millions of people, side effects that can be physically and emotionally devastating, protocols that sometimes prolong suffering unnecessarily, unequal access based on geography and class, conflicts of interest in research, overdiagnosis, etc.
These are complex and important issues that can be resolved with more high-quality science, transparent research, public investment in palliative care, more equitable health policies, and rigorous health regulations. These are problems that require sophisticated, evidence-based solutions implemented through transparent, democratic processes. And they definitely cannot be resolved with conspiracy theories that ultimately enrich modern-day crooks and kill people like Paloma Shemirani.
This story was originally published by Revista Questão de Ciência in Brazil. It is translated and reprinted here with permission.